Paul Manley Back Pain and RSI Clinic
Paul Manley, M.A.O.(Manip), Registered Osteomyologist
RSM (Royal Society of Medicine)
Specialist in the treatment of Musculo-skeletal problems
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line
21/07/2026
Case 1:
 An
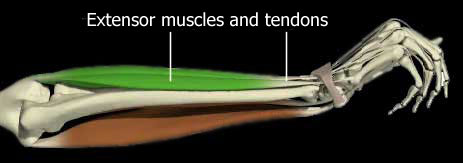
ex-pro-cricketer, this young pianist was experiencing pain along
the line of the extensor tendons of the forearm. It had been building
up for months and was now threatening his playing ability on a
fundamental level.
An
ex-pro-cricketer, this young pianist was experiencing pain along
the line of the extensor tendons of the forearm. It had been building
up for months and was now threatening his playing ability on a
fundamental level.
Findings:
Of athletic build his general muscle tone was higher than I would normally see in a musicians body. This extended to the muscles which were responsible for his symptoms. The deep extensors were very tense and starving themselves of Oxygen because of the restriction to blood flow due to the extreme increased tone in the muscles.
Following one treatment and a couple of follow-up sessions, he made a complete recovery and went on to gain an Honours degree and succesfully competed in many high level music competitions.
Case 2:
 An
awkward fall on to the left hand had resulted in an injury which
had prevented performance for a year in this fiddle player. The
problem was very specific and involved great pain when trying to
play high notes with the little finger, trills and prolonged sustains
being the main aggravators.
An
awkward fall on to the left hand had resulted in an injury which
had prevented performance for a year in this fiddle player. The
problem was very specific and involved great pain when trying to
play high notes with the little finger, trills and prolonged sustains
being the main aggravators.
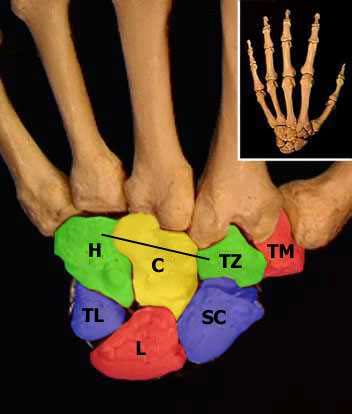
Pain and inflammation resulted on the back of the hand around the area of the Hamate/Capitate/metacarpal joints.
Findings:
The Capitate had turned on its horizontal axis and the upper portion was now 'sticking up', thereby irritating the ligaments binding it as well as the extensor tendon of the little finger which passes over it. See the diagram below: the black line is the horizontal axis of the Capitate. The red area ( illustrated left ) was the centre of irritation.
Following two months of treatment the condition subsided and she is now able to function fully.
 Case
3:
Case
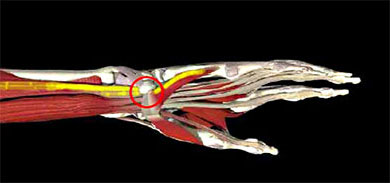
3: Following a fall on to the right hand some months previously, this young cellist experienced great pain in the area of the lateral side of the wrist. (Spread of pain in yellow in figure on the right). She was incapable of 'bowing' for anything other than short periods.
Findings:
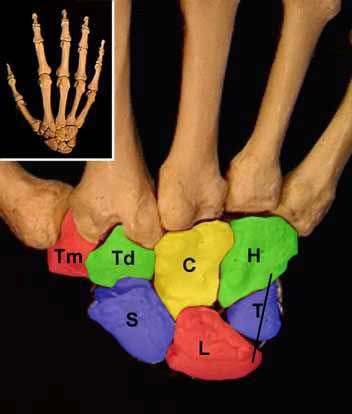
The
Triquetral bone was displaced, having rotated on its vertical axis
( see left diagram ). Its lateral edge was prominent and although
there was some mobility between it and its neighbours, it remained
in a relatively depressed position. This gave rise to mild inflammation
in the joint and the tendons which pass over it on the palmar side.
The result for 'bowing' was profound difficulty.
Following three treatments, full function was restored and remains to this day.
Case 4:
A
tear of the attachment of the extensor tendon to the tip of the
left little finger had resulted in complete loss of function and
inflammation of the joint.
A guitar player, he could no longer use the digit.
extensor tendon to the tip of the
left little finger had resulted in complete loss of function and
inflammation of the joint.
A guitar player, he could no longer use the digit.
Findings:
Three months after the injury, some exostosis or 'outgrowth' of bone had occured resulting in some moderate deformity of the joint. Strength was very weak and the tendency to re-injure was very high.
Following several treatments over a three month period strength and mobility had returned. After specific finger exercises the patient now has more strength than ever before and the problem no longer exists.
Case 5:
A fall on to the left hand 2 years previously had left this fiddle player unable to play or write ( she was left-handed ) and with a continual ache in the wrist joint and up the flexor and extensor tendons with transient pins and needles in the fingertips. She was in extreme distress and had given up on her career, once a renowned performer.
The Scaphoid and lunate joints with the Radius and Ulna were impacted and their ranges of movement reduced by 95 %. The long flexor tendons of the thumb were inflammed at the region of the wrist joint. The deep flexor and extensor tendons were on high tension and their associated muscle portion was overtoned and very dense.
Following four sessions, movement was regained, the areas were much more comfortable and playing rehab commenced. Three months later she was playing again. Within six months she was able to return to the rigours of a full shedule.
 Case
6:
Case
6:
A busy professional pianist, in his late 20's had stiff fingerjoints which were becoming progressively more arthritic. Mobility and speed, deftness and rhythmic control were all affected badly.

Findings:
Most
of the finger joints were slightly swollen, some more than others.
The worst joints were prone to getting exczema over them. The patient
said that the excema usually preceded the joint aggravation.
50% of the joints had 'crystals' of calcium salts grinding roughly
within them. The joint shapes had retained their normal shapes.
Following six treatments over three months the fingers had progressively improved as had the exczema. Twenty years on and he is still playing at the top of his league.
Case 7:
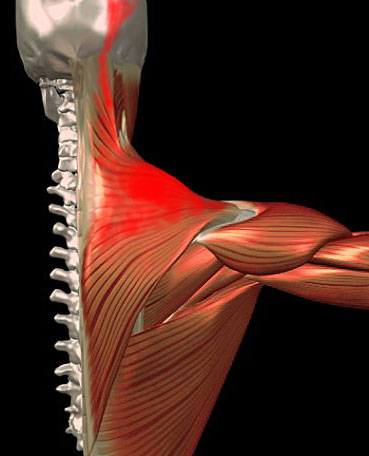
A professional fiddle player had been suffering from great muscle tension in the upper shoulder/neck area. This was triggering headaches and caused great muscle fatigue whilst trying to play.
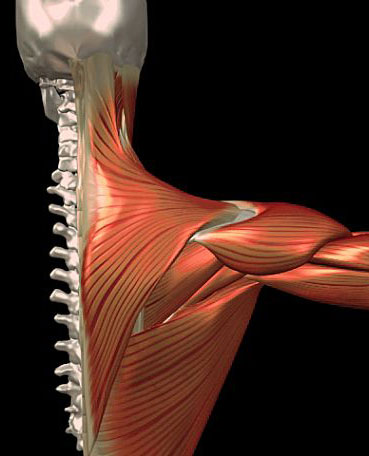
Findings:
The upper fibres of Trapezius had the consistency of 'spongy leather'. They had also undergone a degree of contracture or 'shortening. The tension pattern had spread up as far as the cranium and was accompanied by a major Atlas displacement.
Following three treatments over two weeks, great improvement was noted and playing was easy again.
07925 616 753
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line