Paul Manley Back Pain and RSI Clinic
Paul Manley, M.A.O.(Manip), Registered OsteomyologistFor muscle and joint problems

RSM (Royal Society of Medicine)
Specialist in the treatment of Musculo-skeletal problems
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line
21/07/2026
The neurological control of respiration
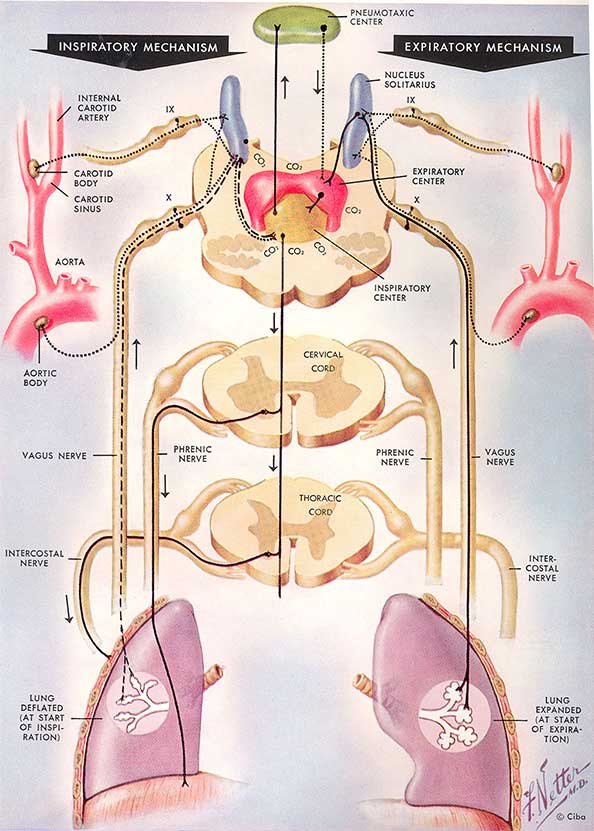
At least three
stimuli are effective in respiratory control and are indicated in
this illustration:
(I) C02, bathing the respiratory center directly (and acting, perhaps, by influencing the actual reaction of the blood),
(2) the chemical composition of the circulating blood, acting on the chemoreceptors in the carotid and aortic bodies, and (3) the degree to which the lung is distended.
The motor neurons to the phrenic nerve (in C4 and C5), to the intercostal muscles (in the thoracic segments, particularly the upper half) and presumably those to the auxiliary muscles of respiration are under the control of an expiratory and an inspiratory center in the medulla oblongata, approximately at the level of the inferior olive. These centers are in the "reticular substance" and appear to be a part of the inhibitory and the facilitatory centres described by Magoun and Rhines.
These two respiratory centers, in their turn, receive afferent fibers from the pneumotaxic center near the hypothalamus and from the solitary nucleus. The latter is under the influence of the messages sent by the chemoreceptors of the carotid body over the glossopharyngeus (IX) and vagus (X) nerves, and by the stretch receptors in the lung sent over the vagus.
When the lung is collapsed (expiration, left half), impulses traveling from stretch receptors over the vagus to the solitary nucleus have a low frequency. They are picked up by the inferior portion of the solitary nucleus and are relayed, probably via the reticulospinal tract and motor neurons in the spinal cord, to the inspiratory centre which then causes the diaphragm and external intercostal muscles to contract.
Expansion of the lung in (inspiration, right half) stimulates the stretch receptors, and impulses are sent along the vagus at high frequency. They are now picked up by a more superior portion of the solitary nucleus which relays impulses to the expiratory center; the latter inhibits the inspiratory muscles and may, in exceptional circumstances, also 'stimulate the expiratory muscles.
This mechanism appears sufficient in itself to insure the play of alternate inspiration and expiration. Chemoreceptors and C02 provide additional security by changing the threshold of response of the neurons composing the respiratory centers.
Although this sounds rather complex, you can think of it like a series of see-saws all making each other go up and down. A primary factor in the settings of the respiratory centre is the stretch settings established by the total lung capacity and the way that we use it. For example, if we breathe in a shallow manner we will gradually reduce the elasticity of the lungs, thereby affecting the sensitivity of the respiratory centre. This in turn can lead to apnoeic breathing disorders such as sleep apnoea and panic attacks.
07925 616 753
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line